
Alternative Approach in Colorectal Anastomotic Stricture: Bougie Dilatation
 Abstract views: 179
/
Abstract views: 179
/  PDF downloads: 145
PDF downloads: 145
DOI:
https://doi.org/10.58600/eurjther1920Keywords:
Anastomotic stricture, colorectal surgery, bougie dilatationAbstract
Dear Editor,
Anostomotic stricture (AS) is seen in 2-30% of patients after colorectal surgery. Various factors such as tissue ischaemia, anastomotic leakage and radiotherapy have been suggested in its pathogenesis [1,2]. Endoscopic methods (balloon dilatation, bougie dilatation, stents, endoscopic electroincision), digital dilatation, surgical methods (stapler stricturoplasty, transanal circular stapler resection, transabdominal redo-anastomosis) and corticosteroids are used in AS [3,4]. Surgery is generally preferred in complete/near complete AS [1]. Stents; the benefit of stents in AS after oncological surgery has not been shown [3]. However, Philip BC Pangg et al. treated near-total AS non-operatively with the colonic/rectal endoscopic ultrasound (EUS) anastomosis technique and a hot lumen metallic stent [5]. We applied 3-stage bougie dilation to the patient with near complete anastomotic stricture.
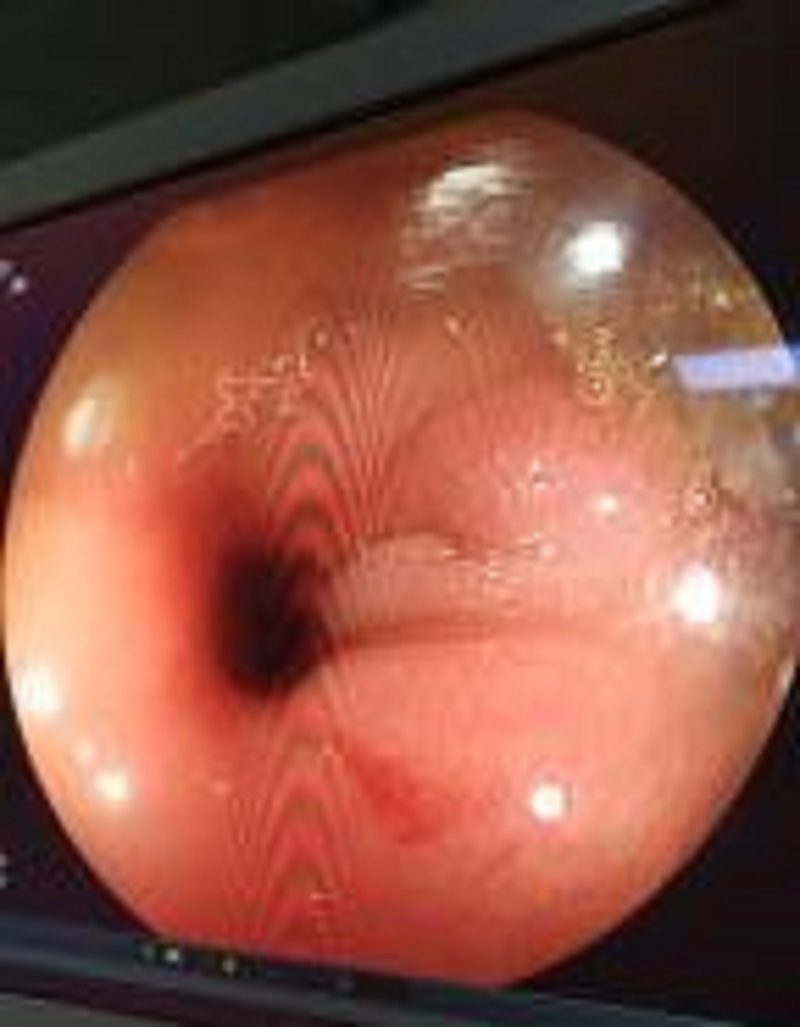
A 59-year-old female patient who underwent laparoscopic anterior resection due to sigmoid colon tumor was followed up with complaints of abdominal swelling, intermittent abdominal pain and difficulty in defecation. One month later, when colonoscopy was performed, near complete anastomotic stricture was observed. Bougie dilatation was performed with maloney flexible bougie dilators under wire guidance. Bougie dilatation was performed 3 times with fifteen days intervals. After the first (33, 36 and 42 F) and the second bougie dilatation (36, 42 F), the upper segment of the anastomotic stricture was reached by gastroscopy. After dilatation with a bougie (42, 45 F) for the third time, the colonoscope was easily passed through the anastomosis line to the upper segment. Six months later, colonoscopy was performed and the proximal part of the anastomosis was easily passed without the use of bougie dilators.
Balloon dilatation is the first method used in AS. However, several repetitions are necessary for the success of the procedure. In addition, the risk of perforation increases when the stricture diameter is <5 mm and length >1 cm. The chances of success in AS are lower compared to bougie dilatation. Endoscopic electroincision is recommended in failure of balloon dilatation. Digital dilatation: used in distal anorectal anostamotic strictures. Corticosteroid application: very large studies are not available. Bougie dilatation in AS provides tactile feedback, allowing the amount of resistance to the passage of the dilator to be estimated and perforation to be avoided. Bougie dilatation method is simple, inexpensive and low risk of complications. Especially Maloney flexible silicone bougie minimise the risk of complications. Bougie dilatators can remain intact for many years and can be reused. But balloon dilatators are not reused. Surgical methods are used in 3-4% (complete/near complete AS) in the failure of endoscopic methods. But mortality risk is high [1,4-6]. Therefore, the alternative method of Philip BC Pang et al. can be applied [5]. However, due to limited endoscopic ultrasonography (EUS) centers, gradual dilatation can be performed with flexible bougie dilators in case of anastomosis stricture.
Yours Sincerely
Metrics
References
Yuan X, Liu W, Ye L, Wu M, Hu B. (2019) Combination of endoscopic incision and balloon dilation for treatment of a completely obstructed anastomotic stenosis following colorectal resection: A case report. Medicine. 98(26);e16292. https://doi.org/10.1097/MD.0000000000016292
Kypraios D, Manthopoulou E, Dimitroulopoulos D, Plastiras A, Ioannou A, Katsinelos D, Tsamakidis K. (2021) A Modified “Rendezvous” Technique for EUS-guided Recanalization of a Rectal Anastomotic Stricture without Fluoroscopy and Stenting. J Gastrointestin Liver Dis. 30(3):404-406. https://doi.org/10.15403/jgld-3792
Clifford RE, Fowler H, Manu N, Vimalachandran D. (2021) Management of benign anastomotic strictures following rectal resection: a systematic review. Colorectal Dis. 23(12):3090-3100. https://doi.org/10.1111/codi.15865
Kashkooli SB, Samanta S, Rouhani M, Akbarzadeh S, Saibil F. (2015) Bougie dilators: simple, safe and cost-effective treatment for Crohn’s-related fibrotic anal strictures. Can J Surg. 58(5):347-8. https://doi.org/10.1503/cjs.001315
Pang PBC, Chouhan A, Joshi HMN, Wheeler JMD, Corbett GD, Varghese S, Godfrey EM. (2023) Endoscopic ultrasound-guided colo-colostomy for the treatment of benign complete occlusion of colonic anastomosis: a case series and description of technique. Colorectal Dis. 25(8):1708-1712. https://doi.org/10.1111/codi.16649
Kraenzler A, Maggiori L, Pittet O, Alyami MS, Prost À la Denise J, Panis Y. (2017) Anastomotic stenosis after coloanal, colorectal and ileoanal anastomosis: what is the best management? Colorectal Dis. 19(2):O90-O96. https://doi.org/10.1111/codi.13587
Downloads
Published
How to Cite
License
Copyright (c) 2023 European Journal of Therapeutics

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
The content of this journal is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






